50 Y/F with Fever since one month and Vomitings since 7 days
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
CHIEF COMPLAINTS:-
50 year old female came with complaints of fever since 1 week associated with vomitings
HISTORY OF PRESENT ILLNESS:-
Patient was apparently asymptomatic 30 days back then she developed fever of high grade with chills and rigors for which she got admitted in hospital and treated , fever relived on medication.
Since 1 week she developed fever of high grade with chills and rigors, continuous relieved on medication but recurring after 3-4 hrs, generalised weakness present, dry mouth present.
Vomitings present 2-3 episodes per day since 1 week , non bilious, projectile, contain food particles, 1 episode of bilious vomiting today morning, nausea present, loss of apetite present.
Pt also have complaints of Right shoulder pain since 1 month with bilateral knee pain since 6 months.
Right shoulder pain associated with restriction of movement and Not associated with morning stiffness.
No h/o loss of weight, sore throat, cough, cold, abdominal pain , diarrhea, burning micturition.
PAST HISTORY:-
N/k/c/o DM, HTN, Thyroid, Asthma, CAD, CVA, Epilepsy
FAMILY HISTORY:-
Insignificant
PERSONAL HISTORY:-
Occupation:- Daily wage worker,used to work for 8-10 hrs and now she has stopped working since one month due to fever and body pains.
Diet:- Mixed
Bowel and Bladder:- Regular
Appetite lost since 1 week
No known allergies
Addictions:- Tobbacco (Chewable)for 1 year, stopped one month back.
Attained menopause 5 months back.
GENERAL EXAMINATION:-
Patient is conscious , coherent & co-operative
Moderately built and nourished.
No signs of pallor, icterus, clubbing, cyanosis, pedal edema and lymphadenopathy.
Vitals @ admission
Temp - 99.2F
RR -18CPM
PR - 132BPM
BP - 140/80mmHg
Spo2 - 99% RA
SYSTEMIC EXAMINATION:-
Respiratory system:-
Bilateral air entry present
NVBS heard
Cardiovascular system:-
S1, S2 heard
CNS:-
NFND
Abdomen:-
Soft, Non tender
Clinical Images:-





INVESTIGATIONS:-
Hemogram

CUE

LFT

Blood urea

Serum Creatinine

Serum Electrolytes

RBS

Uric acid

CRP

ESR

Serology 





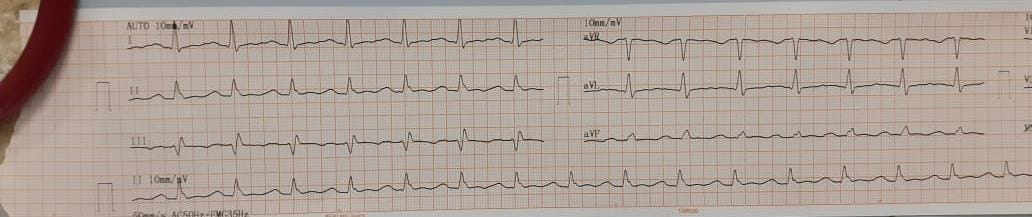
ECG




2D Echo

Chest X ray:-

Right knee X ray(AP and lateral view):-

Left Knee X ray(AP and lateral view):-

Right Shoulder X ray(AP and Axillary view) :-



PROVISIONAL DIAGNOSIS:-
Pyrexia under evaluation
TREATMENT:-
On 11/5/23:-
1)IV fluids NS, RL @ 75ml/hr
2) Inj. neomol 1g/IV/SOS (If temp >101°F)
3) Inj. Zofer 4mg/PO/SOS
4)Tab. PAN 40mg PO/OD
5)Tab.Dolo 650mg PO/BD
6)Temp monitoring 4th hrly
7) Vitals monitoring 4th hrly
On 12/5/23:-
Ortho refferal done on 12/5/23 I/V/O b/l knee pain since 6 months and right shoulder pain since 1 month and advised Tab.Febuxostat 40mg OD for one month and Tab.Hifenac -P for 5 days
Cardiology refferal done on 12/5/23 I/V/O ECG changes and advised Tab.MET XL 25 mg OD

1)IV fluids NS, RL @ 75ml/hr
2) Inj. neomol 1g/IV/SOS (If temp >101°F)
3) Inj. Zofer 4mg/PO/SOS
4)Tab. PAN 40mg PO/OD
5)Tab.Dolo 650mg PO/BD
6) Tab.MET-XL 25mg OD 9 AM
7) Tab.Febuxostat 40mg PO/OD
8)Temp monitoring 2nd hrly
9) Vitals monitoring hrly



Comments
Post a Comment